Research advances from the National Institutes of Health (NIH) Intramural Research Program (IRP) often make headlines. Read the news releases that describe our most recent findings:
Findings in mice point to potential therapies for blinding eye disease uveitis and multiple sclerosis
Researchers at the National Eye Institute (NEI) have identified, isolated, and characterized a unique population of B cells that tamps down the immune system, reducing chronic inflammation. Infusions of purified IL-27 regulatory B cells (I27-Breg ) reduced symptoms in mouse models of multiple sclerosis (MS) and the eye disease autoimmune uveitis. The research suggests the cells may play a role in future human therapies. NEI is part of the National Institutes of Health.
“We are the first to describe this unique population of regulatory B cells. While similar in function to other Bregs, I27-Breg have a distinct gene expression profile and originate from the innate B-1a cell lineage,” said Charles Egwuagu, Ph.D., M.P.H., who directs the NEI Molecular Immunology Section. He and colleagues published their findings in PNAS.
Uveitis is a group of sight-threatening inflammatory eye diseases that includes Behcet disease, birdshot retinochoroidopathy, and sympathetic ophthalmia. Of infectious or autoimmune origin, it is characterized by repeated cycles of intraocular inflammation. Current therapies include corticosteroids; however, prolonged use of these drugs risks other eye problems such as optic neuropathy andsteroid-induced glaucoma.
Photographs of mouse retina showing the effect of uveitis treatment with i27-Bregs. The left column represents a normal retina. Photos in the middle and right column are retinal images from mice with uveitis, untreated or treated with i27-Bregs. The central spot is the optic nerve head. Note the absence of inflammation (ring surrounding the optic nerve) in the IL-27-treated retina (top right image).
NPC1 leads to difficulty controlling movements, liver and lung disease, impaired swallowing, intellectual decline and death
Riluzole, a drug approved to treat amyotrophic lateral sclerosis (ALS), a disease affecting nerve cells controlling movement, could slow the gradual loss of a particular brain cell that occurs in Niemann-Pick disease type C1 (NPC1), a rare genetic disorder affecting children and adolescents, suggests a study in mice by scientists at the National Institutes of Health.
NPC1 results from an impaired ability to move cholesterol through cells, leading to difficulty controlling movements, liver and lung disease, impaired swallowing, intellectual decline and death. Much of the movement difficulties in NPC1 result from gradual loss of brain cells known as Purkinje neurons. The researchers found that mice with a form of NPC1 have a diminished ability to lower levels of glutamate — a brain chemical that stimulates neurons — after it has bound to a neuron’s surface. High levels of glutamate can be toxic to cells. The researchers believe the buildup of glutamate contributes to the brain cell loss seen in the disease. Riluzole blocks the release of glutamate and hence delays the progression of ALS in people.
In the current study, mice with NPC1 survived 12% longer when treated with riluzole, compared to untreated mice. The researchers believe that riluzole or similar drugs may provide a way to slow disease progression in patients with NPC1.
Lung autopsy and plasma samples from people who died of COVID-19 have provided a clearer picture of how the SARS-CoV-2 virus spreads and damages lung tissue. Scientists at the National Institutes of Health and their collaborators say the information, published in Science Translational Medicine, could help predict severe and prolonged COVID-19 cases, particularly among high-risk people, and inform effective treatments.
Although the study was small — lung samples from 18 cases and plasma samples from six of those cases — the scientists say their data revealed trends that could help develop new COVID-19 therapeutics and fine-tune when to use existing therapeutics at different stages of disease progression. The findings include details about how SARS-CoV-2, the virus that causes COVID-19, spreads in the lungs, manipulates the immune system, causes widespread thrombosis that does not resolve, and targets signaling pathways that promote lung failure, fibrosis and impair tissue repair. The researchers say the data are particularly relevant to caring for COVID-19 patients who are elderly, obese, or have diabetes—all considered high-risk populations for severe cases. Study samples were from patients who had at least one high-risk condition.
Colorized scanning electron micrograph of a cell infected with a variant strain of SARS-CoV-2 virus particles (blue), isolated from a patient sample.
NIH scientists say the approach may be a novel way to treat pneumonia in humans
Researchers at the National Institutes of Health have discovered a therapy that targets host cells rather than bacterial cells in treating bacterial pneumonia in rodents. The method involves white blood cells of the immune system called macrophages that eat bacteria, and a group of compounds that are naturally produced in mice and humans called epoxyeicosatrienoic acids or EETs. The research was published in the Journal of Clinical Investigation.
According to the World Health Organization, pneumonia caused by Streptococcus pneumoniae, or pneumococcal pneumonia, is the leading cause of pneumonia deaths worldwide each year. While physicians usually prescribe antibiotics to treat this severe lung infection, treatment is not always successful, and in some cases, the bacteria become resistant.
To keep tissues healthy, EETs work to limit inflammation, but during infections caused by S. pneumoniae and other microorganisms, inflammation ramps up after lung cells induce certain substances that prompt macrophages to gobble up the bacteria. Edin and colleagues found that one way to get macrophages to eat more bacteria is to decrease the ability of EETs to do what they normally do, which is limit inflammation.
Colorized scanning electron micrograph of a macrophage.
Young children with a history of eating problems in the first three years of life were more likely to receive low scores on assessments of child development, according to a study by researchers at the National Institutes of Health. The findings suggest that children with multiple eating problems — frequent crying during meals, pushing food away, gagging and others — may benefit from screening for developmental delay. Early diagnosis of developmental disorders is key to getting children the help they need.
Researchers analyzed data on more than 3,500 children from Upstate KIDS, a study of children born between 2008 and 2010 in New York State. Mothers responded to questionnaires, rating their children’s eating patterns and developmental milestones when the children were 18, 24 and 30 months old. Compared to children who did not have eating problems, children who scored high on eating problems at one or two time points were more than twice as likely to miss a developmental milestone. Children with feeding problems at all three ages were four or more times as likely to miss a milestone.
NIH research highlights importance of data-driven approach to identify novel drug targets
Existing and emerging cancer drugs could be repurposed as therapies to be tested in clinical trials for people at genetic risk of Alzheimer’s disease, according to a new study published in Science Advances. Research combining analysis of brain protein alterations in these individuals as well as laboratory experiments in animal models and cell cultures could help scientists identify existing drugs to test for their potential as Alzheimer’s interventions more quickly.
The findings represent efforts from researchers at the National Institute on Aging (NIA), part of the National Institutes of Health; and NIA-supported teams at the University of California, San Francisco; Rush University, Chicago; and the Icahn School of Medicine at Mount Sinai, New York City.
The scientists identified brain protein changes related to the APOE4 genetic risk variant in young postmortem study participants (average age at death was 39 years) and compared these changes with those in the autopsied brains of people with Alzheimer’s and those without (average age at death was 89 years).
Suicide risk among lesbian, gay, and bisexual adults varies considerably depending on the intersection between sexual identity and other aspects of identity, such as gender, age, and race/ethnicity, according to a study led by researchers at the National Institute of Mental Health (NIMH), part of the National Institutes of Health. The study, which examined data from a nationally representative survey of adults in the United States, also showed that lesbian, gay, and bisexual adults are overall more likely to report suicide-related thoughts, plans, and attempts within the past 12 months compared with heterosexual adults.
The findings, published in the American Journal of Preventive Medicine, indicate that the intersection of multiple social identities may compound suicide risk for some lesbian, gay, and bisexual individuals.
“This study demonstrates the importance of asking about sexual identity in national data collection efforts, and it highlights the pressing need for suicide prevention services that address the specific experiences and needs of lesbian, gay, and bisexual adults of different genders, ages, and race and ethnic groups,” said Rajeev Ramchand, Ph.D., Senior Advisor on Epidemiology and Suicide Prevention at NIMH and lead author of the study.
Scientists at the National Institutes of Health have found that a process in cells may limit infectivity of SARS-CoV-2, and that mutations in the alpha and delta variants overcome this effect, potentially boosting the virus’s ability to spread. The findings were published online in the Proceedings of the National Academy of Sciences. The study was led by Kelly Ten Hagen, Ph.D., a senior investigator at NIH’s National Institute of Dental and Craniofacial Research (NIDCR).
Since the coronavirus pandemic began in early 2020, several more-infectious variants of SARS-CoV-2, the virus that causes COVID-19, have emerged. The original, or wild-type, virus was followed by the alpha variant, which became widespread in the United States in early 2021, and the delta variant, which is the most prevalent strain circulating today. The variants have acquired mutations that help them spread and infect people more easily. Many of the mutations affect the spike protein, which the virus uses to get into cells. Scientists have been trying to understand how these changes alter the virus’s function.
“Throughout the pandemic, NIDCR researchers have applied their expertise in the oral health sciences to answer key questions about COVID-19,” said NIDCR Director Rena D’Souza, D.D.S., Ph.D. “This study offers fresh insights into the greater infectivity of the alpha and delta variants and provides a framework for the development of future therapies.”
Colorized scanning electron micrograph of chronically infected and partially lysed cells (green) infected with a variant strain of SARS-CoV-2 virus particles (blue), isolated from a patient sample.
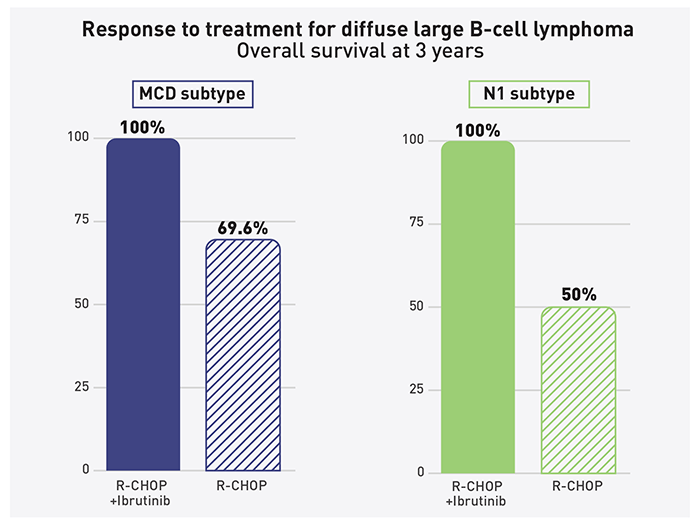
New evidence suggests that adding the targeted therapy ibrutinib (Imbruvica) to a standard chemotherapy regimen can improve how long some younger people with a specific form of diffuse large B-cell lymphoma (DLBCL) live. The findings, published Nov. 4, 2021, in Cancer Cell, come from a new analysis by researchers at the National Cancer Institute (NCI), part of the National Institutes of Health, of a previously conducted phase 3 clinical trial.
Initial results from that study, known as the PHOENIX trial, showed that combining ibrutinib with the standard chemotherapy regimen did not help patients with a form of DLBCL called non-GCB DLBCL to live longer overall. However, by analyzing tumor biopsy samples from patients on the trial, NCI researchers and their collaborators have now shown that younger patients with specific genetic subtypes of non-GCB DLBCL, called MCD and N1, had an exceptional response to the treatment combination, with all such patients alive without disease three years after diagnosis.
“People thought the trial didn’t work,” said Louis M. Staudt, M.D., Ph.D., chief of the Lymphoid Malignancies Branch in the Cancer for Cancer Research at NCI. “But there was something interesting going on — if you just considered younger patients under the age of 60, they had a real benefit from ibrutinib, and we now understand why.”
Younger patients with specific genetic subtypes of non-GCB DLBCL, called MCD and N1, had an exceptional response to the treatment combination.
Different mechanisms suppressed the virus in each person
Research led by scientists at the National Institutes of Health has identified two distinct ways that people with HIV can control the virus for an extended period after stopping antiretroviral therapy (ART) under medical supervision. This information could inform efforts to develop new tools to help people with HIV put the virus into remission without taking lifelong medication, which can have long-term side-effects.
The study involved two adults with HIV who began ART soon after acquiring the virus and continued with treatment for more than six years, successfully suppressing HIV. The individuals then joined an HIV clinical trial and stopped taking ART under medical supervision. The study team followed one of these people for four years and the other for more than five years, with study visits roughly every two to three weeks.
Scanning electron micrograph of an HIV-infected H9 T cell, colorized in Halloween colors.